A common misconception is that the ketogenic diet increases “bad” cholesterol levels and clogs your arteries because it is so high in fat. However, much of the recent research shines light on how high-fat, low-carb diets can optimize your cholesterol levels and in fact improve your heart health.
In this article, we will take a closer look at the most up-to-date research on different types of cholesterol, how each one affects our health, and the impact that the keto diet has on our cholesterol levels.
Cutting through the Fat: What are Lipids and Cholesterol?
Before we can examine the research, we need to understand the roles fat, cholesterol, and carrier molecules called lipoproteins play in the body.
Fats, also known as lipids, are a diverse group of molecules with a “non-polar” characteristic that repels water. This means that you if you put a fat (such as oil or grease) in water, they will not mix.
In the human body, fats are most commonly found in the bloodstream in one of two forms. The first is triglycerides, a fatty acid that stores energy for later use.
These long molecules can be broken down into other fatty acids and glycerol to create fuel for the body. Glycerol can further be broken down and converted into glucose. Elevated levels of triglycerides in your blood can increase your risk of developing diabetes, cardiovascular illnesses, and other life-threatening diseases. [1]
The other important class of lipids in the body is a waxy substance called cholesterol. These molecules have a variety of functions in your body such as building hormones including estrogen and testosterone, maintaining the integrity of cell membranes, and aiding in the absorption of vitamins.
Your body produces all the cholesterol you need in the liver and other cells throughout the body. Cholesterol is also obtained by consuming animal-based foods such as poultry, dairy, and red meat. Typically, 75% of the body’s cholesterol is produced endogenously (internally) while the other 25% is ingested from external sources. [2]
Cholesterol is most commonly transported in the blood by molecules composed of fat and protein called lipoproteins. From least dense to most dense, they come in five forms: chylomicrons, very-low-density lipoproteins (VLDL), intermediate-density lipoproteins (IDL), low-density lipoproteins (LDL), and high-density lipoproteins (HDL). Because VLDL, LDL, and HDL cholesterol are frequently used as clinical indicators, we are going to focus on them.
It is important to emphasize that while they are often referred to as “VLDL cholesterol”, “LDL cholesterol”, and “HDL cholesterol”, these molecules themselves are not cholesterol; they are cholesterol transporters.
What is HDL Cholesterol?
HDL cholesterol is frequently known as “the good cholesterol.” In addition to transporting cholesterol around the body, HDL collects cholesterol that is not being used by cells and brings them back to the liver to be recycled or destroyed.
By doing this, HDL prevents cholesterol from accumulating and clogging arteries. Thus, elevated levels of cholesterol are integral in maintaining optimal cardiovascular health. [3] HDL is typically measured through an HDL-C test, which shows the concentration of cholesterol bound to HDL. Clinically acceptable levels of HDL cholesterol are 40-60 mg/dl and 50-60 mg/dl for women. [4] HDL levels above 60 mg/dl are ideal as they lower the risk of cardiovascular illnesses. [4]
Additionally, HDL cholesterol may have anti-inflammatory effects. A recent research study published by De Nardo et al shows that HDL may be responsible in reducing inflammatory activity by regulating immune system cells called macrophages. [5] Furthermore, epidemiological studies have noted an inverse association between levels of HDL and certain forms of cancer. [6, 7]
More research needs to be performed to investigate the source of these relationships as well as the molecular mechanisms through which HDL operates. However, there is a general consensus among clinicians and scientists that HDL-cholesterol is healthy for the body and that higher levels of HDL-C are healthy for the body. [8] In fact, one study observed that, with every 1 mg/dL reduction in HDL cholesterol, diabetes risk increased by 4%. [9]
Keto and Cholesterol: A Ketogenic Diet’s Connections with Cholesterol
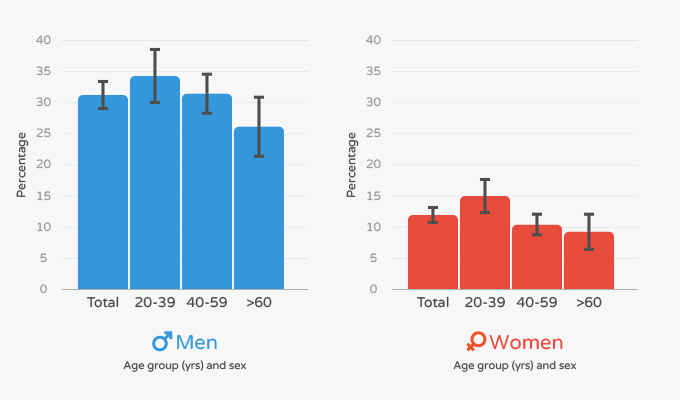
About 32% of men and 13% of women in the US suffer from low levels of HDL cholesterol. [10] Additionally, the majority of Americans do not have HDL cholesterol levels high enough to decrease the risk of cardiovascular illness. [10]
As chronic conditions such as diabetes and cardiovascular illness increase in prevalence worldwide, scientists have evaluated methods to increase levels of HDL cholesterol. For many years, physicians have used drugs called statins to increase HDL (and lower other forms of cholesterol).
Recently, scientists have looked at utilizing dietary interventions as cost-effective methods to optimize HDL cholesterol and prevent the onset of cardiovascular diseases. Below we document three research studies examining low-carb and ketogenic diets effects’ on HDL.
The Impact of Carbohydrate Restriction on HDL Cholesterol
In a recent meta-analysis published in the British Journal of Nutrition by Bueno et al, researchers investigated the impacts of very-low-carbohydrate ketogenic diets (VLCKD) on key metrics of cardiovascular health including HDL cholesterol.
The authors defined a VLCKD as a diet lower in 50g of carbohydrates – lower than the daily recommended grams of carb consumption clinicians recommend to diabetics. They included 13 randomized controlled studies with a total of 1,415 subjects. All studies took place for at least a full year and all subjects included were over 18 years old and had a BMI of at least 27.5 kg/m2. In each of these studies, VLCKD diets were compared to low-fat diets.
Overall, 12 studies including 1257 patients examined the impact of a VLCKD on HDL cholesterol. When assessing the data, the individuals assigned to a VLCKD achieved an average increase in HDL of 0.12 mmol/L. This was double the average increase in HDL of the low-fat dieters who achieved an average increase in HDL of 0.06 mmol/L. [11] As a result, the authors concluded that carbohydrate-restricted diets confer cardiovascular benefits because they improve levels on HDL in the body. [11]
Key Takeaways: A low-carb diet (<50g carb) is an effective method in raising HDL cholesterol when compared to traditional weight-loss diets that emphasize reducing fat intake.
Recommendation: If you need to increase levels of heart-healthy HDL cholesterol, a carbohydrate restricted diet can be an effective tool.
Long-Term Impact of Ketogenic Carbohydrate Restriction on HDL Cholesterol
In a study from 2009 by Brinkworth et al., researchers recruited 118 obese men and women and separated them into two groups for a year-long intervention study. The first group consumed a very-low-carbohydrate, high-saturated diet with 4%, 35%, and 61% energy from carbohydrates, proteins, and fats respectively.
This equates to about 20 grams of carbohydrates on a 2000 kcal diet per day – a more stringent application of carbohydrate restriction use than the meta-analysis above. The second group consumed primarily a low-fat diet with 46%, 24%, and 30% energy from respectively from carbohydrate, protein, and fat per day. Both diets contained an equal number of calories.
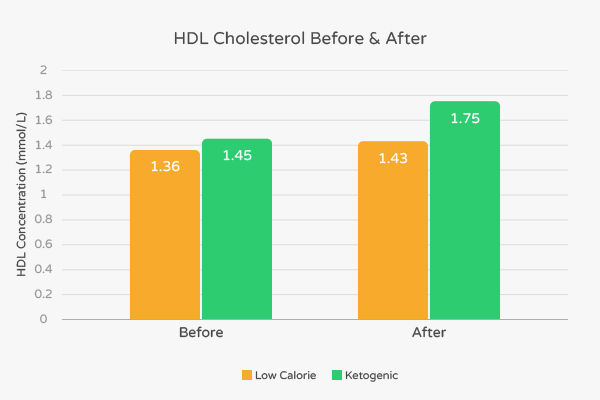
About 59% of participants completed the 12-month trial: 33 in the low-carb group and 36 in the low-fat group. Both groups lost similar amount of body weight and body fat. The subjects who participated in the low-fat intervention experienced an average increase in HDL cholesterol of 0.07 mmol/L from 1.36 mmol/L to 1.43 mmol/L. [12] This represents a 4.9% increase.
In contrast, the subjects who participated in the high-fat intervention experienced an average increase in HDL cholesterol of 0.30 mmol/L from 1.45 mmol/L to 1.75 mmol/L. [12] This represents a 20.6% increase – almost four times as much as that found in the low-fat diet.
Because of their findings, diets very low in carbohydrates may have cardio-protective effects compared to low fat diets.
Key Takeaways: Very low carbohydrate ketogenic diets (<20g Carbs) increase HDL levels substantially more than low fat diets do.
Recommendation: If you need to increase your HDL levels, a ketogenic diet can be a useful dietary intervention.
Carbohydrate Moderation Increases HDL in Healthy, Non-Whites
The majority of studies assessing the effects of carbohydrate restriction on HDL have been conducted on primarily Caucasian, obese subjects.
In 2006, researchers sought to investigate the relationship between carbohydrate intake and HDL cholesterol in a healthy, diverse population. Scientists examined data from Canadians of South Asian, Chinese, European, and Aboriginal origin from two cross-sectional studies conducted in the late 90s.
They included participants who were 35-75 years of age and who were not born in Canada but had lived there for at least 5 years. Subjects who suffered from moderate to severe medical conditions such as diabetes, heart diseases, and active cancer were not included. Subjects of all different weights and BMIs were included as long as they were considered healthy.
Scientists then randomly selected 619 subjects who met these inclusion criteria and examined their carbohydrate intake and levels of HDL cholesterol.
After adjusting for demographic factors such as age, sex, and ethnicity and lifestyle factors such as smoking, researchers noted that subjects in the lowest third of carbohydrate consumption had significantly higher levels of HDL cholesterol than subjects in the highest third of carbohydrate consumption.
More specifically, subjects in the lowest third of carbohydrate consumption had an HDL concentration of 1.21 mmol/L while subjects in the highest third had HDL concentration of 1.08 mmol/L. [13] According to the authors, “every 100-g/d increment of carbohydrate (approximately the difference between the top and bottom tertiles) was associated with 0.15-mmol/L less of HDL.” [13]
Fewer servings of sugary drinks were also associated with higher levels of HDL. [13] Because of their findings, the researchers attributed differences in HDL concentration to carbohydrate intake.
Key Takeaways: Lowering carbohydrate intake is an effective method to increase HDL levels in healthy, non-obese people of all different ethnicities and races.
Recommendation: If your HDL is low and you are eating a high amount of carbohydrates, lowering carbohydrates consumption can increase your HDL cholesterol back to healthy levels. You can accomplish this through a variety of low-carbohydrate diets, including the ketogenic diet.
LDL Cholesterol: Clearing the Confusion
The story behind LDL, or low-density lipoprotein, is more complicated. LDL transports cholesterol produced by your liver and cells throughout your body. Unlike HDL, LDL molecules move slowly through the bloodstream and are vulnerable to oxidizing agents known as “free radicals.” Once oxidized, LDL can easily burrow itself into the walls of your arteries (called endothelium) and impede cardiovascular function. This triggers an inflammatory response in which white blood cells called macrophages rush to eat up the LDL.
Typically known as the “bad cholesterol” to its healthy counterpart HDL cholesterol, increased levels of LDL cholesterol are associated with an increased risk of cardiovascular diseases (CVD). [14] Some studies show a strong correlation between LDL cholesterol and the risk of cardiovascular diseases in both men and women. [15] Evidence also suggests that decreasing blood levels of LDL-C reduces the risk of CVD. [16]
Recent research paints a more intricate picture of this peculiar molecule and has called into question the statement that elevated LDL cholesterol is bad for you. This is for two main reasons. First, LDL can be measured in two ways. The first is called LDL-C which measures the concentration of cholesterol transported by LDL in the blood.
The second is called LDL-P which measures the number of LDL particles in the blood. Sometimes, there is a correlation – more LDL particles means that you can have higher levels of LDL-C. However, larger LDL molecules can grow and carry more cholesterol – leading to a discordance in which LDL-C and LDL-P are not necessarily proportional. When this happens, LDL-C and LDL-P are said to be “discordant.”
For many years, LDL-C tests have been used as the primary method of measuring LDL in the blood. It is cheaper and easier to measure. Recent research has called into questioning how effective LDL-C is compared to LDL-P in precisely assessing cardiovascular risk. After reviewing cross-sectional data, a recent peer-reviewed paper from the world-renowned Framingham Heart Study stated that
“In a large community-based sample, LDL-P was a more sensitive indicator of low CVD risk than either LDL-C or non-HDL-C, suggesting a potential clinical role for LDL-P as a goal of LDL management.” [16]
Another paper produced by the Framingham Heart Study touched upon the difference of LDL-P and LDL-C as indicators.
“…the group with the highest risk for cardiovascular events had high LDL-P and LDL-C, while the group with the lowest risk had low LDL-P but higher LDL-C.” [17]
Collectively, these findings suggest that LDL particle size is a more precise indicator of future cardiovascular illness than total LDL cholesterol even when people have high levels of one but not the other. That being said, LDL-C is still a useful indicator for future cardiovascular illness and ideally you want to have both low LDL-C and LDL-P. (Click here to find optimal ranges for LDL-C and here for LDL-P)
Second, the type of LDL cholesterol you have can lead to different clinical outcomes. LDL can come in different forms – each with different effects on your health. A research study from 1988 showed that having elevated levels of small, dense LDL is three times more likely to lead to heart disease than normal LDL [18].
Thus, larger LDL particles are considered to be healthier for the body. Additionally, more recent research shows that oxidation of LDL by substances called free radicals increases the risk of cardiovascular illness [19].
Finally, there is another, more dangerous lipoprotein called very low-density lipoprotein (VLDL). Like LDL, VLDL transports cholesterol produced by the cells and liver throughout the body. However, VLDL particles also serve as the main transporters of triglycerides in the body.
Additionally, they are composed of higher lipid and lower protein content than LDL. Because of their physical properties and functional purposes, VLDL particles are more likely than other lipoproteins to clog vessels and impair vascular functions. Research studies have noted that high levels of VLDL are associated with increased risk of artherosclerosis and cardiovascular diseases. [20] VLDL is also considered to be a more precise indicator than LDL-C for a variety of metabolic conditions. [21]
Now, we went over a lot about LDL cholesterol, so let’s summarize the key points:
- Low-density lipoprotein (LDL) carries cholesterol throughout the body.
- The sum of the cholesterol in the body attached to cholesterol is called LDL cholesterol (LDL-C).
- The number of LDL particles in the body is referred to as LDL-P.
- LDL-C tests are affordable, general indicators of the risk of cardiovascular disease.
- LDL-P tests are more precise indicators than LDL-C of the risk of cardiovascular disease.
- Smaller, dense LDL cholesterol is more harmful than larger, higher volume LDL cholesterol.
- Very-low Density Lipoprotein (VLDL) carries triglycerides and increased levels of it are strongly associated with greater cardiovascular risk.
LDL and Carbohydrate Restriction: What is the Relationship?
Let’s go back to the research assessing how the low-carb, high-fat diets such as the ketogenic diet affect your LDL levels. In the meta-analysis by Bueno et al., low-carb diets were shown to increase HDL twice as much as low-fat diets after randomized controlled interventions. It also showed that there was a small increase in LDL-C in low-carb subjects compared to low-fat diet subjects who experienced no increase.
The research study by Brinksworth et. al also showed that low-carb diets yielded greater increases in HDL cholesterol when compared to a low-fat diet.
Key Takeaways: Some research suggests that high-fat, ketogenic diets can increase LDL-C by a small amount.
Ketogenic Diet’s Impact on V-LDL Cholesterol and LDL Particle Count
Provided the research showing an increase in LDL levels in human subjects after a low-carbohydrate diet, what does the research say about extreme carbohydrate restriction on V-LDL and LDL particle count?
In a 2006 study, researchers assessed the effects of carbohydrate restriction on LDL cholesterol in a group of 29 men for a 12 week weight-loss intervention. The subjects’ ages ranged from 20-69 years their BMIs ranged from 25 kg/m2 to 30 kg/m2.
Their intervention diets consisted of 10% of energy from carbohydrates, 65% of energy from fat, and 25% of energy from protein. Assuming a 2000 kilocalorie diet, this translates to approximately 50 grams of carbohydrates daily.
After the 12 weeks intervention, researchers noted that the concentration of LDL particles decreased by 9.6% from 1180 nmol/L 1180 to 1066 nmol/L. [22] As previously mentioned, lower levels of LDL particles are beneficial to cardiovascular fitness. Additionally, the particle size of LDL increased by an average of 5.2% from 20.75 mm to 21.27 mm. [22]
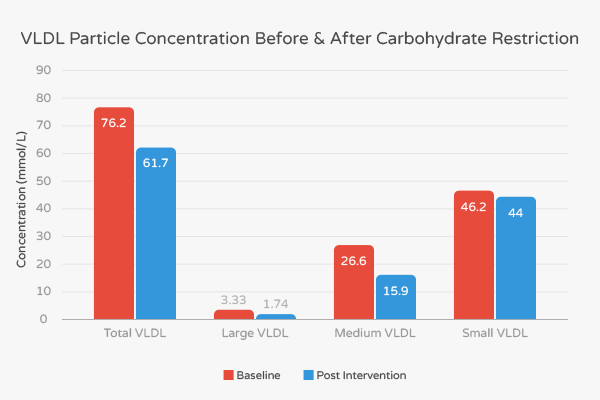
Researchers also observed that the size of VLDL particle size did not change in either of the groups. However, they noted that the total number of VLDL particles decreased by 19% from 76.2 nmol/L to 61.7 nmol/L. [22] More specifically, large VLDL particles reduced by 40.2% from 3.33 nmol/L to 1.74 nmol/L, medium VLDL particles decreased by 4.8% from 46.2 nmol/L to 44 nmol/L. [22]
Because of these favorable effects on LDL particle concentration, LDL particle size, and quantity of VLDL particles, the scientists concluded that
“…weight loss induced by carb restriction favorably alters the secretion and processing of plasma lipoproteins, rendering VLDL, LDL, and HDL particles associated with decreased risk for atherosclerosis and coronary heart disease.” [22]
Another study in primarily adult, female subjects showed similarly promising results. In a randomized, parallel clinical trial, researchers recruited 119 subjects for a 6 month long intervention. The mean age of the subjects was 44.9 years, their mean BMI was 34.4 kg/m2, and 76% were women.
59 of the subjects were randomized to a low-calorie ketogenic diet which included a nutritional supplementation of borage, fish and flaxseed oil. The second group of 60 consumed a reduced-calorie diet.
After the intervention, researchers noted that the ketogenic diet group had decreased their VLDL by 78%, their medium VLDL by 60%, and their small VLDL by 57%. [23] Additionally, their large LDL had increased by 54%, medium LDL decreased by 42%, and small LDL decreased by 78%. [23] Overall, the average particle size increased by 2% and the LDL particle concentration decreased by 11%. [23]
This optimization in LDL cholesterol was less pronounced in the low fat group compared to the low-carb ketogenic diet group. It is important to mention that LCKD did not lower total LDL cholesterol. However, as mentioned previously, two studies by the Framingham Heart Study indicate that LDL-P is a stronger indicator than LDL-C. [16, 17]
In fact, one study stated that “…the group with the highest risk for cardiovascular events had high LDL-P and LDL-C, while the group with the lowest risk had low LDL-P but higher LDL-C.” [17] As a result of prior clinical research and their findings, the researchers stated that: “While the low carb, ketogenic diet did not lower total LDL cholesterol, it did result in a shift from small, dense LDL to large, buoyant LDL, which could lower cardiovascular disease risk.” [23]
From this, we can conclude that a low-carb, ketogenic diet helps you optimize your LDL cholesterol.
Key Takeaways: Low carbohydrate diets help reduce the number of LDL and VLDL particles and increase the size of LDL particles in overweight people. These all have positive effects on cardiovascular fitness.
Recommendation: If you have high levels of LDL particles and VLDL particles, consider adopting a carbohydrate-restricted diet. To optimize your LDL cholesterol levels, consider adopting a diet high in healthy monounsaturated fats.
Why The Ketogenic Diet Optimizes Cholesterol Levels: The Impact of Specific Fatty Acids
Now that we know about the effect that the ketogenic diet has on cholesterol levels — a finding that seems to contradict everything we thought we knew about cholesterol and fat — let’s find out how such a high-fat diet actually optimizes cholesterol levels.
The most convincing piece of evidence can be found in a 2003 meta-analysis. In this meta-analysis, researchers compiled the data from sixty trials that quantified the effect that feeding different types of fats to humans had on the total-to-HDL cholesterol ratio [25]. But before we look through the results, we must first understand what this ratio is.
The total-to-HDL cholesterol ratio is found by dividing your total cholesterol level by your HDL-C, and it is essentially the same thing as an LDL-to-HDL cholesterol ratio since most non-HDL cholesterol is LDL cholesterol [26]. The researchers of the 2003 meta-analysis used this ratio because it is a better cardiovascular risk predictor than total cholesterol levels [25].
Now that we have a superficial understanding of the total-to-HDL cholesterol ratio, let’s look at the results of the meta-analysis. The two findings that the researcher’s highlight most are the effects that lauric acid (found in high quantities in coconut oil) and stearic acid (found in high quantities in animal fats) have on the total-to-HDL cholesterol ratio. Both of these fatty acids improved the total-to-HDL cholesterol ratio more favorably than carbohydrates [25]. (A similar pattern emerges for blood sugar and triglyceride levels when we replace carbs with fat as well.)
The researchers also found that unsaturated fats, especially polyunsaturated fats, decreased (improved) the ratio. However, lauric acid has a more favorable effect on the total-to-HDL cholesterol ratio than any other fat, saturated or unsaturated.
Because of these findings, we can infer that the low-carb, high-fat diet optimizes cholesterol levels for two main reasons:
- Replacing carbs with the fats that are commonly consumed on the ketogenic diet improve total-to-HDL cholesterol ratio.
- Eating more unsaturated fats and lauric acid help to improve cholesterol levels even further.
In other words, when you restrict carbohydrates and get a majority of your calories from animal fats, coconut oil, and unsaturated fats like fish, nuts, avocado, and olive oil, it is highly likely that you will improve your cholesterol levels. One of the best ways to incorporate all of this into one diet plan is by following the ketogenic diet.
However, it is important to take these results with a grain of salt. The authors of this 2003 meta-analysis suggest that we use this data to inform the hypotheses of controlled trials so that we can directly test the effects that each dietary fat has on heart disease risk.
Key Takeaways: By replacing carbohydrates with stearic acid, lauric acid, monounsaturated fats, and polyunsaturated fats, total-to-HDL cholesterol ratio improves.
Recommendation: If you are looking to optimize your cholesterol levels and reduce your cardiovascular disease risk, a ketogenic diet that mainly consists of coconut oil, olive oil, avocados, nuts, fish, and animal fats may work best for you. (Still concerned about the recent claims that coconut oil is bad for you? Our article on coconut oil will help clear up the confusion.)
Practical Application: How to Interpret The Cholesterol Levels on Your Blood Test Results
The beneficial effects that the ketogenic diet has on cholesterol levels are not guaranteed for everyone. This is why it is important to consult your doctor and get your blood tested to track the results of your dietary changes.
Most of your blood test results, however, may only cause more confusion. Your LDL-C, HDL-C, Total cholesterol, and triglycerides numbers are valuable, but they only provide small pieces to the puzzle of your cardiovascular health. Does this mean that you have to get an advanced cholesterol panel?
Although some doctors may suggest it if you have genetic factors that are actively contributing to your cardiovascular health, an advanced cholesterol panel isn’t necessary for everyone. Instead, most people should look for a different blood marker that can be found from the results of a standard blood lipid panel — the total-to-HDL cholesterol ratio. Why?
Dr. Chris Masterjohn postulates that this ratio is an accurate marker for the amount of time that LDL particles spend in the blood [26]. This is an important thing to take note of because the LDL particles are more likely to become oxidized and cause atherosclerosis when they are in the blood for longer periods of time. This gives us a deeper explanation of why the authors of the 2003 meta-analysis looked at the total-to-HDL cholesterol ratio rather than total cholesterol levels.
So, what does this mean for you? When you get your blood lipid panel results back, look at your total-to-HDL cholesterol ratio. Dr. Masterjohn suggests that your total-to-HDL cholesterol ratio should be between 3 and 4 to ensure healthy cholesterol levels and a substantially reduced risk of heart disease.
Key Takeaway: Total-to-HDL cholesterol ratio is the best predictor of cardiovascular disease risk on the basic blood lipid panel.
Reccomendation: To verify that the ketogenic diet is improving your cholesterol levels, make sure your total-to-HDL cholesterol ratio is getting lower. Aim for a ratio between 3 and 4.
What if Keto is Making Your Cholesterol Levels Worse?
Although the evidence suggests that the keto diet can help optimize cholesterol in many groups of people, there are others that may not fare well, from a heart health perspective, when they eat a high fat, low carb diet.
One way to tell if the keto diet may not be ideal for you is if your total-to-HDL cholesterol ratio is above 4 and/or your LDL-P remain high or increase after starting the keto diet. If this is the case for you, then it may indicate that you have a particular condition that requires you to make adjustments to your keto diet or follow a completely different diet altogehter. [27]
Here is a brief overview of the most common conditions that can cause cholesterol levels to increase in an unhealthy way on a keto diet:
Familial Hypercholesterolemia
Familial hypercholesterolemia is a condition where one or more of the genes for the LDL receptor are defective. Having the right amount of properly functioning LDL receptors plays a vital role in maintaining healthy cholesterol levels by clearing LDL cholesterol out of the blood. Without an adequate amount of LDL receptors, the blood is much more likely to accumulate high levels of LDL particles, increasing the body’s vulnerability to cardiovascular disease significantly. [28]
If a person with familial hypercholesterolemia is then put on a high-fat diet, they will become even more vulnerable to heart disease as the increased saturated fat and cholesterol content of the diet provokes higher cholesterol levels. And it gets even worse — since this person lacks the ability to clear LDL cholesterol out of their blood normally — their cholesterol levels will stay elevated for an even longer period of time. This will make it much more likely that the LDL particles will become damaged and stimulate plaque build up in the blood vessels.
To counteract these genetic vulnerabilities, it is may be best to eat a low to moderate fat diet that is whole food based with plenty of fiber, monounsaturated fats, polyunsaturated fats (especially omega 3s), and limited saturated fats. This, as well as a lifestyle filled with physical activity, stress relief practices, and plenty of sleep, should keep their cholesterol levels under control.
One way to find out if you have some of the genetic variants that lead to familial hypercholesterolemia is to send off a saliva sample to a genetic testing lab (just make sure you buy a testing kit first). Genetic testing companies like 23 and Me test for many of the genetic variants that can cause familial hypercholesterolemia.
However, these tests aren’t completely necessary to find out if a high fat, low carb diet isn’t working well for you. Within a couple of weeks to a month of keto dieting, you should be able to tell if your blood lipids are getting better or worse with a simple blood test and everything you learned throughout this article.
If you find that your blood lipids have gotten much worse or that your total cholesterol-to-HDL ratio is getting further and further from 4, then this indicates that you may have genetic variants that make it difficult for you to deal with higher fat diets.
Is this the case for you? If so, consider adjusting your diet so that it is lower in fat and higher in fiber and carbs with a focus on plant-based foods, while also increasing your physical activity, improving sleep quality, decreasing stress levels, and aiming to maintain a healthy weight.
Hypothyroid Related Issues
Thyroid hormones and cholesterol levels are intimately linked. [30] In fact, thyroid hormone has a powerful influence on LDL receptor expression. The effect is so powerful that it stimulates the LDL receptors in our liver and sex hormone-producing glands to soak up the LDL cholesterol in the blood like a sponge. [28]
Unfortunately, the opposite is true as well. When our thyroid hormone levels are low, our LDL receptors will be less active. This causes LDL cholesterol to stay in the blood for more extended periods of time.
As the LDL cholesterol remains in the blood, it will be much more vulnerable to damage. Once the LDL particles get damaged, they will start to trigger plaque building processes in the blood vessels, increasing the risk of heart disease.
If you have a history of hypothyroid issues, you may also struggle with unhealthy cholesterol levels as well — and the keto diet can make them even worse. However, for those of you who are being treated for your hypothyroid condition or who have an autoimmune thyroid condition, you may be able to follow the keto diet without any problems. In fact, many keto dieters with autoimmune thyroid conditions have found that the keto way of eating improved their quality of life more than any other diet.
Chronic Inflammation and Stress
Both Inflammation and stress elicit similar mechanisms — one of which is an increase in cholesterol levels to bring the necessary nutrients to our tissues to help them heal and recover. [27]
If you have chronic inflammation and/or stress, you may also have persisting high cholesterol levels which, in most cases, isn’t doing anything but causing more problems. The preponderance of this chronic inflammation and stress is typically caused by a variety of lifestyle factors, from eating foods that trigger inflammation to sleeping poorly. [27]
Fortunately, the keto diet has been found to decrease inflammation (which is part of the reason why it can help people who have autoimmune thyroid conditions). [29] However, if you still have high levels of inflammation after following the keto diet, then you may have to address other important variables like your stress levels, sleep quality, and food allergies/sensitivities before your cholesterol levels can rest at healthier levels. (By addressing these variables, you will also decrease your stress levels which may help improve your cholesterol levels even more.)
One way to find out if the keto diet is helping quell your chronic inflammation is by seeing how your C-reactive protein (CRP) levels change over time on your routine blood test. [27] If CRP levels decrease after you’ve made your lifestyle and dietary changes, then you are on the right track. The ideal result is if your cholesterol levels are optimized along with that.
However, for those of you who see a drop in inflammation and a worsening of your cholesterol levels, you may have one of the two issues that we explored earlier.
What to Eat If Your Cholesterol is Rising on the Keto Diet
If the standard keto diet is impairing your cholesterol levels, there are several adjustments you can make to improve heart health without giving up on keto living.
The most effective change is to replace most of your saturated fat intake with minimally-processed sources of monounsaturated and polyunsaturated fats. This simple shift will decrease your consumption of foods that can impair cholesterol levels while emphasizing fats that tend to have a positive effect.
The easiest way to reduce your saturated fat intake is by limiting these foods:
- Coconut oil
- Butter
- Ghee
- Palm oil
- Heavy cream
- Fatty cuts of red meat
- Dark chocolate
Eat the following keto-friendly foods instead:
- Protein sources lower in saturated fat — fish, seafood, poultry, and eggs
- Fats/oils high in monounsaturated fats — extra virgin olive oil, avocado oil, and duck fat for cooking and dressings
- Nuts and seeds — macadamia nuts, brazil nuts, pecans, flaxseeds, and chia seeds are the lowest carb options
- High-fat fruits — avocados and olives
- Full-fat cheese*
- MCT oil* — for a fat and ketone boost
*Though these are high in saturated fat, studies have shown that they don’t increase LDL levels. [31, 32]
Essentially, this is a variation of a ketogenic Mediterranean diet that emphasizes cholesterol-optimizing foods. To learn more about this approach and follow a simple keto meal plan, read through our guide to Mediterranean keto.
Conclusion on a Ketogenic Diet’s Connections with Cholesterol
Cholesterol is a complicated molecule in the body that comes in many different forms – each with varying clinical significance. That said, an abundant amount of research suggests that low-carb, high-fat ketogenic diets have a clinically-positive impact on each form. More specifically:
- Ketogenic diets increase the concentrations of heart-healthy HDL cholesterol more than low-fat, high-carb diets. [11, 12]
- Lowering carbohydrate consumption in healthy individuals also leads to higher levels of HDL cholesterol. [13]
- Low-carb, high-fat diets decrease LDL particle concentration (LDL-P) and increase the size of LDL cholesterol. [22, 23]
- Ketogenic diets decrease the amount of harmful VLDL cholesterol in the blood. [22, 23]
How does the ketogenic diet accomplish all of this? Mostly by replacing carbs with fats that reduce the total-to-HDL cholesterol ratio like coconut oil, animal fats, nuts, avocados, olive oil, and fish.
To find out if the ketogenic diet is actually improving your cholesterol levels, check your total-to-HDL cholesterol ratio — researchers suggest that it is one of the best predictors of cardiovascular disease risk. Make sure your total-to-HDL cholesterol ratio is between 3 and 4.
If you find that your cholesterol levels are worsening on a standard ketogenic diet, then replacing some of your saturated fat intake with foods higher in monounsaturated and/or polyunsaturated fats can be helpful. For practical suggestions and tips, feel free to use the food list in the previous section, and read through our Mediterranean keto diet guide.
Overall, the information throughout this article shows that carbohydrate restriction, as emphasized by the ketogenic diet, can be a healthy choice for you.
If you have high cholesterol or have been prescribed statins and are interested in transitioning to a ketogenic diet, one of the easiest ways would be to download our keto meal plan app. This will provide you with a simple meal plan tailored to your needs, preferences, and health goals.
Sources
- Miller, Michael, et al. “Triglycerides and cardiovascular disease a scientific statement from the American Heart Association.” Circulation 123.20 (2011): 2292-2333.
- Johnson, Teddi Dineley. “Mind your cholesterol for a healthy heart.” The Nation’s Health 40.3 (2010): 24-24.
- Barter FJ, et al. Anti-inflammatory properties of HDL. Circulation Research. 2004; 95: 764-772
- “What Do My Cholesterol Levels Mean?” (PDF). American Heart Association. September 2007. Retrieved 14 November 2009.
- De Nardo D, et al. (2014) High-density lipoprotein mediates anti-inflammatory reprogramming of macrophages via the transcriptional regulator ATF3. Nature Immunology. 15,152–160
- Jafri, Haseeb, Alawi A. Alsheikh-Ali, and Richard H. Karas. “Baseline and on-treatment high-density lipoprotein cholesterol and the risk of cancer in randomized controlled trials of lipid-altering therapy.” Journal of the American College of Cardiology 55.25 (2010): 2846-2854.
- Zhao, Wenhui, et al. “HDL Cholesterol and Cancer Risk Among Patients With Type 2 Diabetes.” Diabetes care (2014): DC_140523.
- Barter, Philip, et al. “HDL cholesterol, very low levels of LDL cholesterol, and cardiovascular events.” New England Journal of Medicine 357.13 (2007): 1301-1310.
- Stern MP et al. Ann Intern Med 2002; 136:575-581
- Carroll MD, Kit BK, Lacher DA. Total and high-density lipoprotein cholesterol in adults: National Health and Nutrition Examination Survey, 2009–2010. NCHS data brief, no. 92. Hyattsville, MD: US Department of Health and Human Services, CDC, National Center for Health Statistics; 2012.
- Bueno, Nassib Bezerra, et al. “Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials.” British Journal of Nutrition 110.07 (2013): 1178-1187.
- Brinkworth, Grant D., et al. “Long-term effects of a very-low-carbohydrate weight loss diet compared with an isocaloric low-fat diet after 12 mo.” The American journal of clinical nutrition 90.1 (2009): 23-32.
- Merchant, Anwar T., et al. “Carbohydrate intake and HDL in a multiethnic population.” The American journal of clinical nutrition 85.1 (2007): 225-230.
- Germano, Giuseppe, et al. “European Guidelines on cardiovascular disease prevention in clinical practice (version 2012).” European Heart Journal 33 (2012): 1635-1701.
- Neaton, James D., et al. “Serum cholesterol level and mortality findings for men screened in the Multiple Risk Factor Intervention Trial.” Archives of internal medicine 152.7 (1992): 1490-1500.
- Cromwell, William C., et al. “LDL particle number and risk of future cardiovascular disease in the Framingham Offspring Study—implications for LDL management.” Journal of clinical lipidology 1.6 (2007): 583-592.
- Otvos, James D., et al. “Clinical implications of discordance between low-density lipoprotein cholesterol and particle number.” Journal of clinical lipidology 5.2 (2011): 105-113.
- Meisinger, Christa, et al. “Plasma oxidized low-density lipoprotein, a strong predictor for acute coronary heart disease events in apparently healthy, middle-aged men from the general population.” Circulation 112.5 (2005): 651-657.
- Parthasarathy, Sampath, et al. “Oxidized low-density lipoprotein.” Free Radicals and Antioxidant Protocols. Humana Press, 2010. 403-417.
- Adiels, Martin, et al. “Overproduction of very low–density lipoproteins is the hallmark of the dyslipidemia in the metabolic syndrome.” Arteriosclerosis, thrombosis, and vascular biology 28.7 (2008): 1225-1236.
- VanderLaan, Paul A., et al. “VLDL best predicts aortic root atherosclerosis in LDL receptor deficient mice.” Journal of lipid research 50.3 (2009): 376-385.
- Wood, Richard J., et al. “Carbohydrate restriction alters lipoprotein metabolism by modifying VLDL, LDL, and HDL subfraction distribution and size in overweight men.” The Journal of nutrition 136.2 (2006): 384-389.
- Westman, Eric C., et al. “Effect of a low-carbohydrate, ketogenic diet program compared to a low-fat diet on fasting lipoprotein subclasses.” International journal of cardiology 110.2 (2006): 212-216.
- Fuehrlein, Brian S., et al. “Differential metabolic effects of saturated versus polyunsaturated fats in ketogenic diets.” The Journal of Clinical Endocrinology & Metabolism 89.4 (2004): 1641-1645.
- Mensink, Ronald p., et al. “Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials” The American Journal of Clinical Nutrition 77.5 (2003): 1146-1155.
- Masterjohn, Chris. “The Total-to-HDL Cholesterol Ratio — What Does It Mean?” Chris Masterjohn, PhD. 13 January 2009. Retrieved 14 October 2017.
- Masterjohn, Chris. “What to Do About High Cholesterol” Chris Masterjohn, PhD. 19 January 2017. Retrieved 21 May 2018.
- Masterjohn, Chris. “Dietary Management of Heterozygous Familial Hypercholesterolemia (HeFH)” Chris Masterjohn, PhD. 23 January 2016. Retrieved 21 May 2018.
- Masino, Susan A., and David N. Ruskin. “Ketogenic Diets and Pain.” Journal of child neurology 28.8 (2013): 993–1001. PMC. Web. 22 May 2018.
- Rizos, C.V, M.S Elisaf, and E.N Liberopoulos. “Effects of Thyroid Dysfunction on Lipid Profile.” The Open Cardiovascular Medicine Journal 5 (2011): 76–84. PMC. Web. 22 May 2018.
- Cheese intake in large amounts lowers LDL-cholesterol concentrations compared with butter intake of equal fat content — The American Journal of Clinical Nutrition
- Medium Chain Triglyceride Oil Consumption as Part of a Weight Loss Diet Does Not Lead to an Adverse Metabolic Profile When Compared to Olive Oil — NCBI